Case Study: Nonalcoholic Steatohepatitis (NASH)
Case Background:
A 52-year-old male presents to the hepatology clinic after abnormal liver function tests were noted during a routine health check-up. The patient is referred for further evaluation of suspected fatty liver disease.
The clinical team includes a physician, dietitian, and a clinical pharmacist as part of a multidisciplinary care model.
 Patient Demographics
Patient Demographics
|
Parameter |
Details |
|
Age |
52 years |
|
Sex |
Male |
|
Ethnicity |
South Asian |
|
Height |
172 cm |
|
Weight |
92 kg |
|
BMI |
31.1 |
|
Occupation |
Office-based accountant |
|
Alcohol |
Occasional |
|
Smoking status |
Non-smoker |
 Medical History
Medical History
|
Condition |
Duration |
|
Type 2 Diabetes Mellitus |
8 years |
|
Dyslipidemia |
6 years |
|
Hypertension |
5 years |
|
Obesity |
>10 years |
 Current Medication History
Current Medication History
|
Medication |
Dose |
Frequency |
Duration |
|
Metformin |
1000 mg |
Twice daily |
8 years |
|
Glimepiride |
2 mg |
Once daily |
4 years |
|
Atorvastatin |
20 mg |
Once daily |
6 years |
|
Amlodipine |
5 mg |
Once daily |
5 years |
 Presenting Complaints
Presenting Complaints
- Persistent fatigue for the past 6 months
- Mild right upper quadrant abdominal discomfort
- No jaundice, pruritus, or ascites
 Laboratory Investigations
Laboratory Investigations
Liver Function Tests
|
Test |
Patient Value |
Normal Range |
|
ALT (SGPT) |
92 U/L |
7–56 U/L |
|
AST (SGOT) |
78 U/L |
10–40 U/L |
|
ALP |
128 U/L |
44–147 U/L |
|
Total Bilirubin |
0.9 mg/dL |
0.3–1.2 mg/dL |
|
Albumin |
4.1 g/dL |
3.5–5.0 g/dL |
Metabolic Parameters
|
Test |
Patient Value |
Normal Range |
|
Fasting Plasma Glucose |
162 mg/dL |
70–99 mg/dL |
|
HbA1c |
8.4% |
<5.7% |
|
Total Cholesterol |
238 mg/dL |
<200 mg/dL |
|
LDL-C |
152 mg/dL |
<100 mg/dL |
|
HDL-C |
36 mg/dL |
≥40 mg/dL |
|
Triglycerides |
256 mg/dL |
<150 mg/dL |
Additional Tests
|
Test |
Patient Value |
Normal Range |
|
Platelet Count |
210 ×10⁹/L |
150–450 ×10⁹/L |
|
INR |
1.0 |
0.8–1.2 |
|
Serum Creatinine |
0.9 mg/dL |
0.6–1.3 mg/dL |
 Imaging & Histology
Imaging & Histology
|
Investigation |
Findings |
|
Abdominal Ultrasound |
Increased hepatic echogenicity consistent with fatty liver |
|
FibroScan |
Liver stiffness: 9.2 kPa |
|
Liver Biopsy |
Macro vesicular steatosis, hepatocyte ballooning, lobular inflammation; no cirrhosis |
|
Histological Parameter |
Detailed Findings in This Patient |
|
Biopsy adequacy |
Ultrasound-guided percutaneous liver biopsy; specimen length >20 mm with >12 portal tracts identified |
|
Type of steatosis |
Macrovesicular steatosis |
|
Extent of steatosis |
Approximately 55–60% of hepatocytes involved |
|
Distribution of steatosis |
Predominantly zone 3 (centrilobular) with extension into zone 2 |
|
Microvesicular steatosis |
Absent |
|
Hepatocyte ballooning |
Obvious ballooning degeneration present |
|
Ballooning distribution |
Predominantly in zone 3 hepatocytes |
|
Hepatocyte disarray |
Mild to moderate |
|
Mallory–Denk bodies |
Present in scattered ballooned hepatocytes |
|
Lobular (intralobular) inflammation |
Mixed inflammatory infiltrate |
|
Predominant inflammatory cells |
Polymorphonuclear leukocytes with lymphocytes |
|
Severity of lobular inflammation |
>2 inflammatory foci per 200× field |
|
Portal inflammation |
Present |
|
Severity of portal inflammation |
Mild to moderate lymphocytic infiltrate |
|
Interface hepatitis |
Absent |
|
Fibrosis pattern |
Perisinusoidal fibrosis with classic “chicken-wire” appearance |
|
Fibrosis location |
Predominantly zone 3 (centrilobular) |
|
Portal fibrosis |
Mild portal fibrosis present |
|
Bridging fibrosis |
Absent |
|
Cirrhosis |
Absent |
|
Kupffer cell activation |
Present |
|
Apoptotic bodies |
Occasional |
|
Glycogenated nuclei |
Present |
|
Iron deposition |
Absent |
|
Bile duct injury / cholestasis |
Absent |
 CASE-BASED QUESTIONS (Pharmacist-Focused)
CASE-BASED QUESTIONS (Pharmacist-Focused)
Disease Understanding & Assessment
- What features differentiate NAFLD from NASH in this patient?
- Based on the provided clinical, laboratory, and histological data, how would the severity of liver disease be classified?
Pharmacotherapy Decision-Making
- What pharmacological treatment options could be considered for this patient based on current clinical guidelines?
- What patient-specific factors would influence the selection of pioglitazone as a therapeutic option?
- Under what clinical circumstances might vitamin E be considered appropriate in this patient?
Pharmacist’s Clinical Role
- What role does the pharmacist play in evaluating the risk–benefit profile of pioglitazone in this case?
- How can the pharmacist assess potential drug–disease and drug–drug interactions with the current medication regimen?
- What baseline parameters should the pharmacist recommend before initiating therapy?
Safety, Monitoring & Follow-up
- What adverse effects associated with pioglitazone are clinically relevant for this patient?
- What safety concerns should be considered before initiating long-term vitamin E therapy?
Patient Counseling & Adherence
- What counseling points should the pharmacist provide regarding lifestyle modification alongside pharmacotherapy?
Outcome Evaluation
- What clinical and laboratory markers would indicate therapeutic success?
Disease Understanding & Assessment:
- What features differentiate NAFL from NASH in this patient?
NAFL (non-alcoholic fatty liver) and NASH (non-alcoholic steatohepatitis) can easily be differentiated from each other using the following criteria for diagnosis mentioned in the image below:

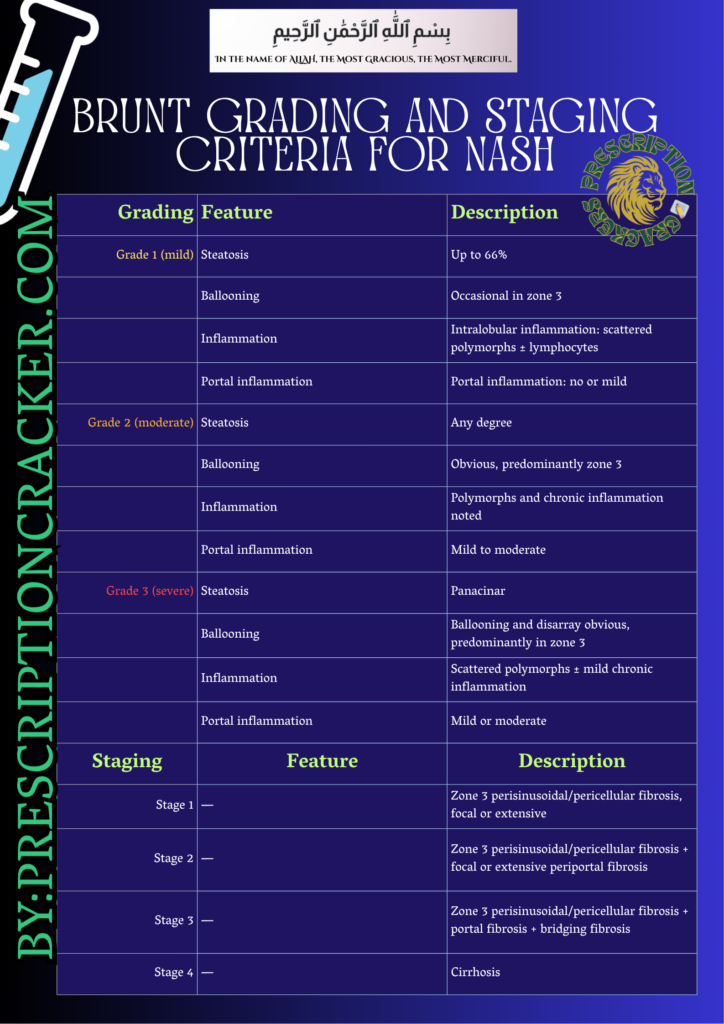
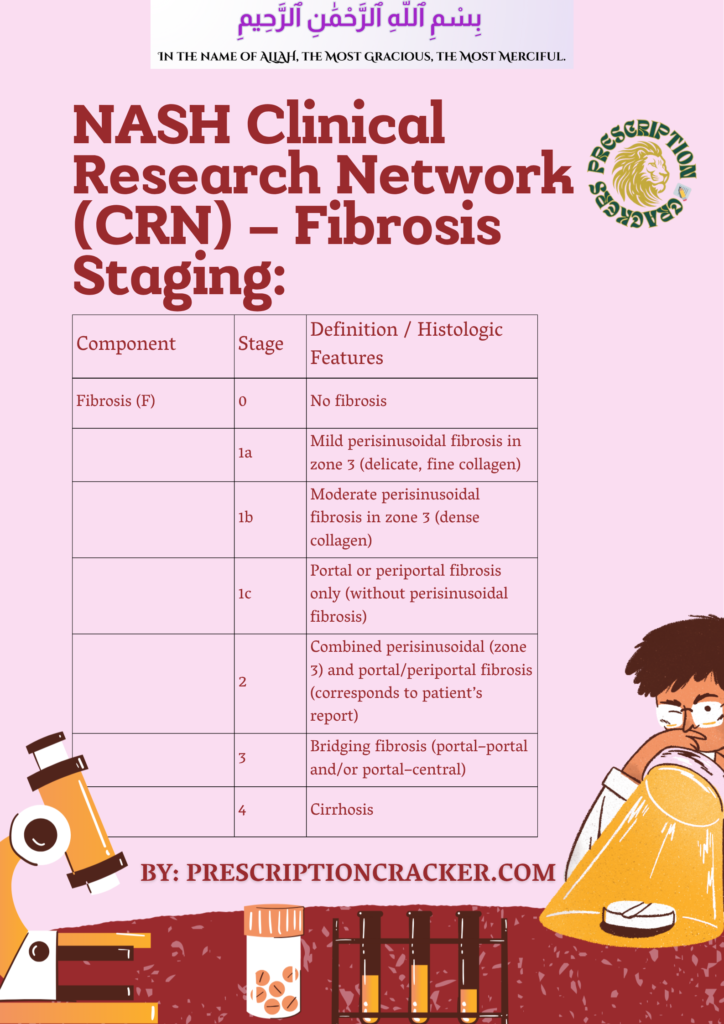
Thus, the patient is estimated to be suffering from stage 2 of fibrosis as per NASH CRN system of fibrosis staging.
3. What pharmacological treatment options could be considered for this patient based on current clinical guidelines?
First-line (cornerstone)
- Weight loss (7–10%)
- Optimized glycemic, lipid, and BP control
Pharmacotherapy Options:
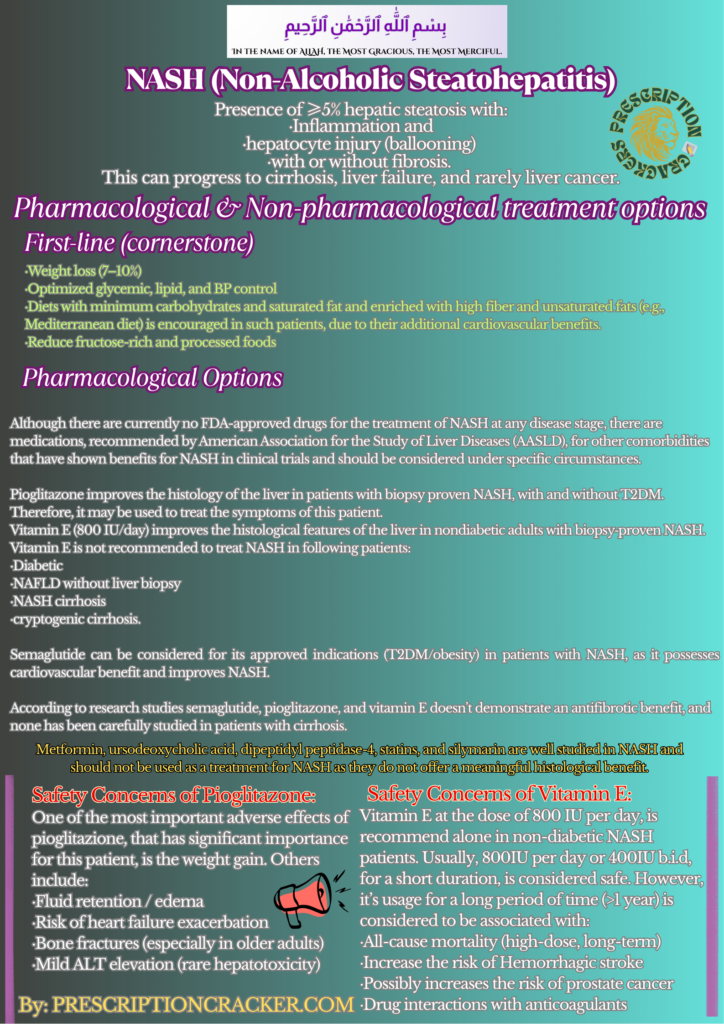
Although there are currently no FDA-approved drugs for the treatment of NASH at any disease stage, there are medications, recommended by American Association for the Study of Liver Diseases (AASLD), for other comorbidities that have shown benefits for NASH in clinical trials and should be considered under specific circumstances.
Pioglitazone improves the histology of the liver in patients with biopsy proven NASH, with and without T2DM. Therefore, it may be used to treat the symptoms of this patient.
Vitamin E (800 IU/day) improves the histological features of the liver in nondiabetic adults with biopsy‐proven NASH. Vitamin E is not recommended to treat NASH in following patients:
- Diabetic
- NAFLD without liver biopsy
- NASH cirrhosis
- cryptogenic cirrhosis.
Semaglutide can be considered for its approved indications (T2DM/obesity) in patients with NASH, as it possesses cardiovascular benefit and improves NASH.
According to research studies semaglutide, pioglitazone, and vitamin E doesn’t demonstrate an antifibrotic benefit, and none has been carefully studied in patients with cirrhosis.
Metformin, ursodeoxycholic acid, dipeptidyl peptidase-4, statins, and silymarin are well studied in NASH and should not be used as a treatment for NASH as they do not offer a meaningful histological benefit.
- What patient-specific factors would influence the selection of pioglitazone as a therapeutic option?
Pioglitazone, a thiazolidinedione derivative, is a peroxisome proliferator–activated receptor γ (PPARγ) agonist), works by increasing insulin sensitivity, which reduces liver inflammation and steatosis as well. Pioglitazone also offers significant histological benefits for NASH patients.
The patient under study is suffering from both the diabetes as well as NASH so, pioglitazone could be selected for this patient as it improves glycaemic control as well as alleviate pathological features of the liver.
FAQ: What is peroxisome proliferator–activated receptor (PPAR)?
PPARs are ligand-activated transcription factors that plays a significant role in the expression of more than 100 genes and affect several metabolic processes, especially lipid and glucose homeostasis.
- Under what clinical circumstances might vitamin E be considered appropriate in this patient?
According to American Association for the Study of Liver Diseases (AASLD), vitamin E (800IU/day) is recommended in the patients with NASH who are non-diabetic. Vitamin E has been shown to improve the histology of liver and associated NASH symptoms.
As per some research studies, the combination of vitamin E and pioglitazone, have shown to improve NASH symptoms in patients with T2DM, and not with the vitamin E alone.
In the case under study, patient is suffering from type 2 diabetes so vitamin E alone couldn’t be considered in this patient. However, combination of pioglitazone with vitamin E as an add-on therapy can be considered in case of persistent necroinflammation, provided there are no contraindications and long-term safety risks are carefully assessed.
- What role does the pharmacist play in evaluating the risk–benefit profile of pioglitazone in this case?
Pioglitazone has been shown to improve the symptoms associated with NASH so, its benefit in this case is can be expected. Research studies have demonstrated that while metabolic improvements might start earlier, liver-specific benefits typically require at least 12 to 18 months of treatment to achieve maximum effectiveness.
Pharmacist should evaluate the following risk factors associated with the usage of pioglitazone:
- Pioglitazone can cause weight gain (averaging roughly 2.5 kg to 4% increase in body weight) and this patient is already suffering from obesity. So, daily exercise to reduce weight is essentially recommended to this patient before initiating pioglitazone.
- Secondly, the patient is already on anti-diabetic medications like metformin and glimepiride, co-administration of another anti-diabetic medication like pioglitazone can cause hypoglycemia. Thus, close monitoring of blood glucose level is recommended to this patient.
- Patient should be screened for:
- Heart failure (NYHA III–IV contraindication: NYHA Classes III and IV represent advanced heart failure, classified by significant functional limitations)
- History of fractures: as pioglitazone has shown to increase the risk of fractures
- Bladder cancer history (controversial but assessed)
- How can the pharmacist assess potential drug–disease and drug–drug interactions with the current medication regimen?
Current Medication History
The current medication of this patient includes the following:
Medication | Dose | Frequency | Duration |
Metformin | 1000 mg | Twice daily | 8 years |
Glimepiride | 2 mg | Once daily | 4 years |
Atorvastatin | 20 mg | Once daily | 6 years |
Amlodipine | 5 mg | Once daily | 5 years |
Drug-Disease interaction:
The pharmacist should assess drug–disease interactions by identifying agents that may worsen metabolic risk factors or hepatic outcomes. Glimepiride, a sulfonylurea, may contribute to weight gain and insulin resistance, potentially exacerbating NASH. Additionally, as it is hepatically metabolized, there is an increased risk of hypoglycemia in liver disease, warranting careful monitoring or consideration of alternative antidiabetic agents. Although uncommon, glimepiride has been implicated in cholestatic liver injury.
Drug-Drug interaction:
As pioglitazone is planned to be initiated in this patient, so it’s noteworthy that it may interact with the other anti-diabetic medications like metformin and glimepiride and can increase the risk of hypoglycemia.
Apart from this, there are no such risk of drug-drug interaction in current regime of this patient.
- What baseline parameters should the pharmacist recommend before initiating therapy?
Following baseline parameters would be recommended by pharmacist before initiating therapy:
- Blood glucose level via HBA1c and fasting glucose
- Liver function test (LFTs)
- BMI
- BP
- Lipid profile
- Baseline edema assessment
- Bone health risk assessment (vitamin D, fracture risk)
- Heart failure screening
- What adverse effects associated with pioglitazone are clinically relevant for this patient?
One of the most important adverse effects of pioglitazione, that has significant importance for this patient, is the weight gain as the patient is already suffering from obesity. Others include:
- Fluid retention / edema
- Risk of heart failure exacerbation
- Bone fractures (especially in older adults)
- Mild ALT elevation (rare hepatotoxicity)
- What safety concerns should be considered before initiating long-term vitamin E therapy?
Vitamin E at the dose of 800 IU per day, is recommend alone in non-diabetic NASH patients. Usually, 800IU per day or 400IU b.i.d, for a short duration, is considered safe. However, it’s usage for a long period of time (>1 year) is considered to be associated with:
- All-cause mortality (high-dose, long-term)
- Increase the risk of Hemorrhagic stroke
- Possibly increases the risk of prostate cancer
- Drug interactions with anticoagulants
- What counselling points should the pharmacist provide regarding lifestyle modification alongside pharmacotherapy?
Pharmacist’s Counselling
- Pharmacist should recommend weight reduction to this patient as he is suffering from obesity (BMI=1 kg/m²), Target should be 7–10% weight loss.
- Diets with minimum carbohydrates and saturated fat and enriched with high fiber and unsaturated fats (e.g., Mediterranean diet) is encouraged in such patients, due to their additional cardiovascular benefits.
- Reduce fructose-rich and processed foods
- Alcohol: strictly avoided
- As per research studies Coffee consumption, irrespective of caffeine content, have demonstrated positive effects especially in liver fibrosis. Taking 3 or more cups per day could be recommended to this patient, if not contraindicated.
- Exercise (≥150 min/week) is also encouraged in such patients. Exercise can also improve frailty, sarcopenia, and quality of life in patients with chronic liver disease.
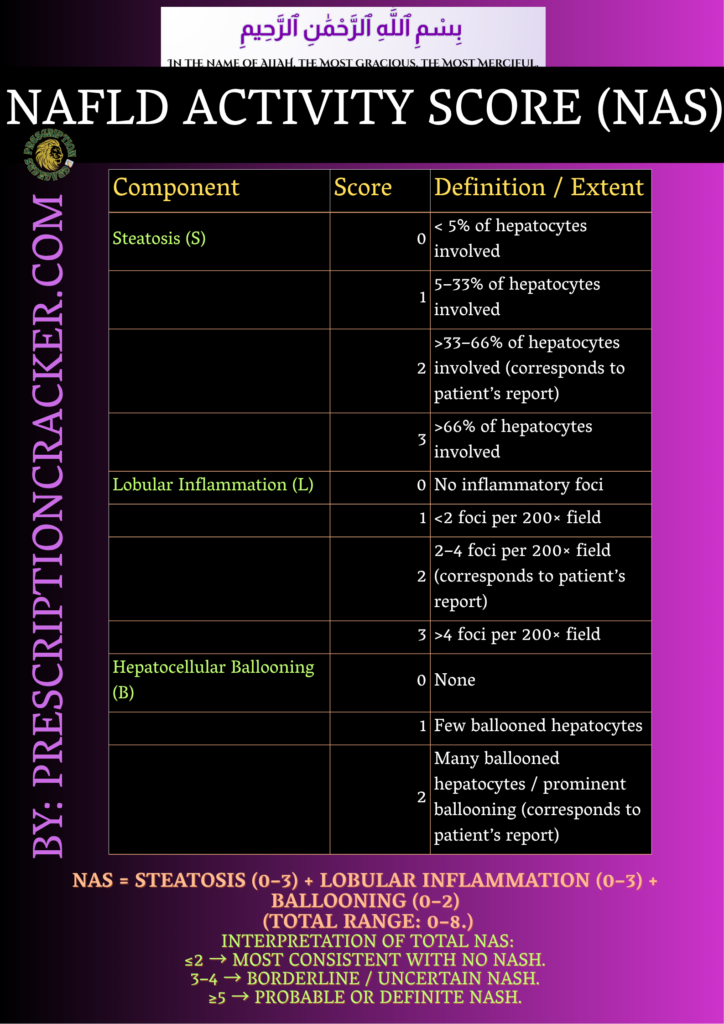
- What clinical and laboratory markers would indicate therapeutic success?
The primary endpoint is often considered as the reduction of at least 2 points on the Non-alcoholic fatty liver disease activity score (NAS) without worsening of fibrosis. Alongside there are some other clinical and laboratory marker that might indicate the therapeutic success.
- Normalization of LFT
- BMI (within 18.5 – 24.9 kg/m²)
- Improvement in glycemic control with HbA1c normalization
- Normalization of cholesterol, LDL, HDL and triglycerides.
- Improvement in results of abdominal ultrasound and Fibroscan (Non-invasive diagnostics).
- Histology (if reassessed): Alleviation of hepatic pathological manifestation in the form of inflammation, hepatic ballooning, steatosis and fibrosis (if present).