 Patient Profile
Patient Profile
- Name: A
- Age: 34 years
- Sex: Female
- Occupation: Digital content creator
- Work Pattern: Prolonged screen exposure (8–10 hours/day)
- Lifestyle: Irregular sleep–wake cycle, limited physical activity
 Chief Complaint
Chief Complaint
- Recurrent episodes of severe headache for the past 4 years, with increased frequency during the last 8 months.
 History of Present Illness
History of Present Illness
- Headache frequency: 5–7 episodes per month
- Character of pain:
- Pulsating
- Unilateral (mostly temporal region)
- Intensity: Moderate to severe
- Duration: 8–36 hours
- Associated symptoms:
- Nausea and occasional vomiting
- Sensitivity to light and sound
- Neck stiffness
- Post-attack fatigue and brain fog
Identified triggers include:
- Missed meals
- Dehydration
- Mental stress
- Hormonal fluctuations
- Poor sleep quality
Past Medical History
- Functional dyspepsia
- Mild iron deficiency treated intermittently
- No history of seizures or chronic systemic illness
Medication History
- Intermittent use of:
- Paracetamol
- Combination analgesics
- No continuous preventive therapy
 Dietary and Hydration History
Dietary and Hydration History
- Inconsistent water intake (≤1.5 L/day)
- Diet low in:
- Fresh vegetables
- Fruits
- Dairy products
- Limited intake of:
- Fish
- Eggs
- Nuts
- Occasional use of multivitamins without regular adherence
 Family History
Family History
- First-degree relative with migraine
- No family history of neurodegenerative disease
 Physical Examination
Physical Examination
- Blood pressure: Normal
- BMI: 22.8 kg/m²
- General examination: Unremarkable
- Neurological examination: Within normal limits
|
Test |
Patient Value |
Normal Reference Range |
|
Hemoglobin (Hb) |
11.1 g/dL |
12.0–15.5 g/dL |
|
Mean Corpuscular Volume (MCV) |
81 fL |
80–96 fL |
|
Serum Ferritin |
14 ng/mL |
15–150 ng/mL |
|
Vitamin B12 (Cobalamin) |
230 pg/mL |
200–900 pg/mL |
|
Serum Folate |
4.2 ng/mL |
4.0–20.0 ng/mL |
|
Plasma Homocysteine |
16 µmol/L |
5–15 µmol/L |
|
25-Hydroxy Vitamin D |
18 ng/mL |
30–100 ng/mL |
|
Vitamin A (Retinol) |
0.9 µmol/L |
0.7–2.8 µmol/L |
|
Vitamin E (α-Tocopherol) |
7.5 mg/L |
5.5–17 mg/L |
|
Serum Magnesium |
1.8 mg/dL |
1.7–2.4 mg/dL |
|
Serum Calcium |
9.1 mg/dL |
8.6–10.2 mg/dL |
|
ALT (SGPT) |
22 U/L |
7–35 U/L |
|
AST (SGOT) |
20 U/L |
8–33 U/L |
 Case-Based Questions
Case-Based Questions
- Which water-soluble vitamins could be explored in relation to migraine pathophysiology in this patient?
- Which fat-soluble vitamins may influence neuronal health or inflammatory responses?
- How might hydration status interact with vitamin metabolism and migraine frequency?
- What is the possible link between elevated homocysteine and micronutrient status?
- Which patient-specific factors would guide safe vitamin supplementation?
 Pharmacist Workup:
Pharmacist Workup:
First of all, we need to find out whether these symptoms fit on the criteria of being diagnosed as migraine or not.
So, let’s look at the typical features of migraine:
Typical Migraine Features
- Headache lasting 4–72 hours (with 2 or more of following features)
- Unilateral (one-sided) pain
- Throbbing or pulsating quality
- Moderate to severe intensity
- Worsens with routine physical activity
- Associated with any one or more of following:
- Nausea and/or vomiting
- Photophobia (light sensitivity)
- Phonophobia (sound sensitivity)
Now, if we compare it with the patient’s symptoms, we can easily find out many similarities. It is also noteworthy that no deviations are appeared in neurological examination.
Additionally, to rule out any dangerous headaches, doctors usually look for red flag “SNOOP” Criteria:
Red Flags (Suggest another disorder):
- S: Systemic symptoms (fever, weight loss)
- N: Neurological deficits
- O: Onset sudden (“thunderclap headache”)
- O: Older age (>50 years at onset)
- P: Pattern change or progressive worsening
Absence of these features supports primary headache disorders like migraine.
Now let’s look at the questions asked to solve the case:
- Which water-soluble vitamins could be explored in relation to migraine pathophysiology in this patient?
By looking at the patient’s lifestyle, we came to know that the patient’s diet is low in fruits, vegetables, diary and meat etc which all are rich in vitamin B-complex, So, it can be estimated that the patient would be deficient in the majority of B-complex vitamins.
By looking at the report of the patient, we found out that the homocysteine level of the patient is heigh and serum vitamin B12 and folate level (B9), though not deficient but are also at border line of the normal range
|
Test |
Patient Value |
Normal Reference Range |
|
Hemoglobin (Hb) |
11.1 g/dL |
12.0–15.5 g/dL |
|
Serum Ferritin |
14 ng/mL |
15–150 ng/mL |
|
Plasma Homocysteine |
16 µmol/L |
5–15 µmol/L |
|
Vitamin B12 (Cobalamin) |
230 pg/mL |
200–900 pg/mL |
|
Serum Folate |
4.2 ng/mL |
4.0–20.0 ng/mL |
Hyperhomocysteinemia may be due to:
- MTHFR gene mutation
- MTHFR gene activates the MTHFR enzyme whose one of the functions is Homocysteine Regulation, in which it plays its role via conversion of 5,10-methylenetetrahydrofolate into the active form of folate (5-methylTHF) that is capable of donating methyl group.
- It also Helps using the enzyme Methionine Synthase (MTR) that transfer methyl group from 5-methyltetrahydrofolate (5-methylTHF), requiring Vitamin B12 (cobalamin) to homocysteine, preventing high homocysteine levels, which are linked to cardiovascular issues.
- Other functions of MTHFR enzyme includes: DNA synthesis and repair, methylation, neurotransmitters production and detoxification.
- Vitamin B deficiency (Vitamin B6, B9 & B12 particularly)
As per patient’s case history, there is no mention of MTHFR mutation so, it may be concluded that the patient is deficient in Vitamin B6, B9 and B12. These vitamins can be supplemented to bring down the homocysteine levels, in order to alleviate the symptoms of migraine as hyperhomocysteinemia is one of the risk factors of migraine attacks.
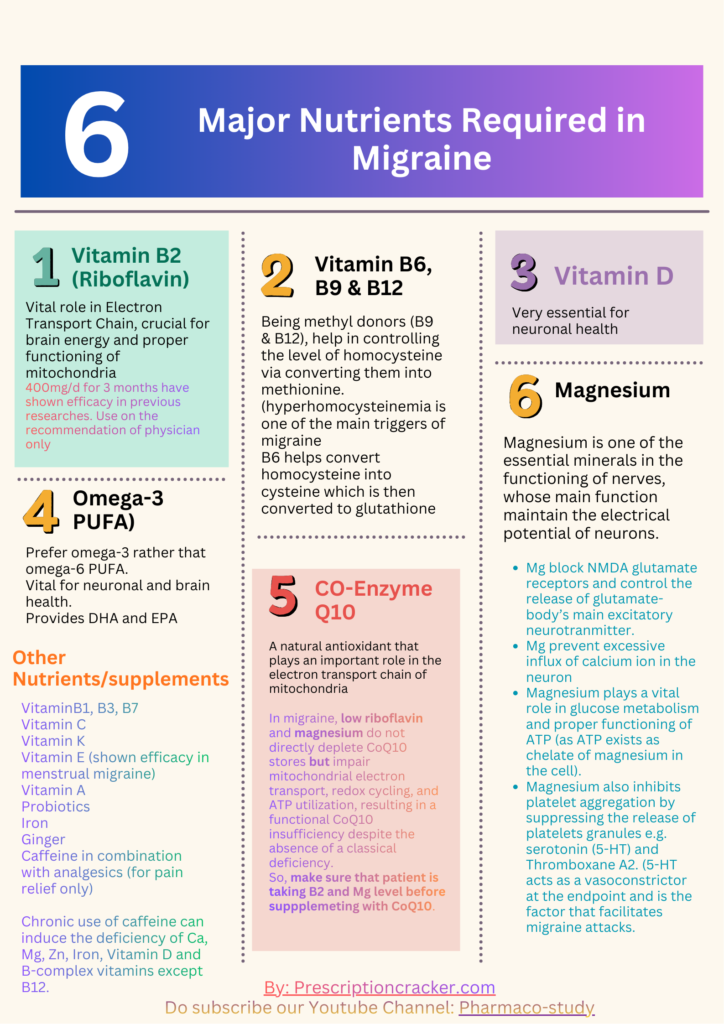
Another important water-soluble vitamin that plays a significant role in the brain functioning is vitamin B2 (Riboflavin). As, we known that the neuroinflammation and disruption in brain energy are among the possible causes of migraine attacks in patient and it is also found out through many research studies that deficiency of riboflavin is associated with the neuroinflammation and consequently migraine attacks in patient.
Riboflavin is one of the vital components of oxidative metabolism due to its role as the precursor to coenzymes, flavin mononucleotide (FMN), and flavin– adenosine–dinucleotide (FAD) in mitochondria. (Discussed further in case study-2)
So, in this case we may recommend riboflavin as well, as the patient’s diet is not enriched with riboflavin containing foods
400mg/day of riboflavin for 12 weeks is proven to be effective for the prevention of migraine attack in the patients.
- Which fat-soluble vitamins may influence neuronal health or inflammatory responses?
Though Vitamin K deficiency is also associated with the nerve spasm and optic nerve damage, but Vitamin D has more significant effect on the neuronal health and prevention of neuroinflammation.
Let’s look at some of the major functions of Vitamin D with regard to the neurons:
The role of vitamin D in some brain functions is well known.
- Calcitriol, the active form of Vitamin D, can affect neuroplasticity, and apoptosis
- Vitamin D, 1-alphahydroxylase (vitamin D-binding protein), and VDR (Vitamin D receptors) are present in different areas of the central nervous system.
- Vitamin D plays significant role in the modulation of cellular oxidative stress levels, intracellular calcium concentration, immune system function, and neurotrophic factor production in the CNS.
- Vitamin D also inhibits the destruction mechanisms of nerve cells. Therefore, the protective role of vitamin D in protecting against neurodegenerative diseases in humans is evident
And as we can see this patient’s lab report is also suggesting low level of Vitamin D, So, Vitamin D supplementation can be given to this patient.
- How might hydration status interact with vitamin metabolism and migraine frequency?
Effect of hydration status on the Metabolism of Vitamins:
The hydration status highly influences the metabolism of not only the vitamins but also the carbohydrate, fats and proteins in the following ways:
- Water constitutes the major portion of saliva that helps in the lubrication of food as well as proper digestion of carbohydrates
- Water especially cold water, via thermogenic effects, causes the body to burn calories in order to raise the temperature of the water as per the body temperature.
- Water solubilizes vitamins especially water-soluble vitamins and minerals which allows easy absorption of water-soluble vitamins and minerals in the body.
So, yes, hydration status of a person highly influences the metabolism of vitamins
Effect of hydration status on Migraine:
Hydration level highly effects the occurrence of migraine. Dehydration has been considered as one of the main triggers of migraine. When the body losses more water than it takes in then the chances of incidence of migraine increases drastically.
When we talk about the loss of water from the body, it doesn’t only mean the water alone rather the water lost from the body also takes salts (sodium & potassium) and glucose with it, which highly affect the electrolyte level of the body consequently causing the disturbance in the osmolarity and electrical activity of brain
FAQ: Can we take juices, sodas, alcohol, or other beverages rather than simple water?
No, it is best to talk pure water rather than juices, sodas, alcohol, or other beverages as such drinks have high osmolarity (salt content) and less water so, they are less hydrating. Even low-calorie drinks or sugar-free drinks also contains aspartame which as per some researches, can trigger migraine attack in some sensitive individuals.
- What is the possible link between elevated homocysteine and micronutrient status?
Homocysteine levels are regulated through one-carbon metabolism, a group of interconnected pathways that transfer single-carbon units needed for normal cellular function. In this system, homocysteine is remethylated to methionine using folate-derived methyl groups with vitamin B12 as a cofactor, leading to the formation of S-adenosylmethionine (SAM), the body’s main molecule that donates methyl groups for DNA, histone, and neurotransmitter methylation. Vitamin B6, while not a direct methyl donor, supports homocysteine clearance through the transsulfuration pathway by converting it to cysteine, thereby preventing homocysteine accumulation and its neurotoxic effects. Thus these vitamins plays an important role in the regulation of homocysteine which keep the level of the homocysteine within the normal range. However, the deficiency of these vitamins can lead to the elevation of the homocysteine in the body. High level of homocysteine can trigger migraine attack and can adversely affect the cardiac functions.
- Which patient-specific factors would guide safe vitamin supplementation?
In this case, vitamin supplementation should be guided by
- Laboratory findings:
The vitamins should be recommended according to the lab reports. Like as we can see that the level of Vitamin A and E are normal so, there is no need to give these vitamins likewise there is a deficiency of iron/ferritin level so, patient must be given a suitable iron supplement that suits his gastric conditions as well. Similarly, the level of Vitamin B9 and B12 are at borderline and the level of homocysteine is high so, the supplementation with vitamin B6, B9 & B12 alongside B2 can be considered.
- Migraine characteristics:
Identification of migraine triggers are important, which we can observe in this case as dehydration, stress, hormonal fluctuation, dietary insufficiency and skipped meals. Secondly, it should be kept in mind that the vitamin supplementation is recommended as preventive medicine not for actively occurring migraine attack.
- Dietary habits:
Patient’s diet is very essential and a natural source of all the vitamins, minerals, protein, & glucose etc. So, primarily the improvement of diet is recommended for this patient before moving to vitamins supplementation, as the vitamins and minerals etc. obtained from diet are much beneficial, easy to absorb and free from added preservatives. Secondly, the hydration status of this patient is also very low, which should be encouraged to improve in order to enhance the absorption and metabolism of vitamins.
- Gastrointestinal tolerance:
Gastrointestinal health status is one of the most important factors to be considered before initiating any oral medicine. In this case, we come to know that the patient is suffering from functional dyspepsia which may be worsen by some vitamins or forms of iron supplements. So, it’s very essential to give gastric friendly formulation of vitamins and iron or to design a diet plan that fulfils the patient’s dietary need while being gentle on stomach.
Secondly, as the functional dyspepsia is linked to the stress, depression and anxiety so, the patient must be counselled in this regard as well.
- Liver function:
Proper functioning of liver is very important for the appropriate metabolism of vitamins especially fat-soluble vitamins. As per the report of this patient, the liver is in healthy state so, the deficient vitamins can be given within the permitted range.
- Lifestyle factors:
Lifestyle factors should be modified in this case like doing physical activity 30min per day, maintaining hydration, avoiding stressful conditions, following 20-20-20 rule while using laptop or screen, and eating fresh fruits, vegetables, meat, fish and eggs etc.
- Safety profile of each vitamin:
Before recommending any vitamin, the lab reports should be considered and if some of the vitamins are in adequate amount especially fat-soluble vitamin then they shouldn’t be added in Vitamin regime. It’s because fat soluble vitamins tend to accumulate in the body and can cause toxicity if given without the body need. Likewise, the water-soluble vitamins, though the excess is eliminated through kidney, should be given as per body need and within the safe limits to avoid any adverse effects.